

Four years ago, researchers warned the Centers for Medicare and Medicaid Services that some doctors were overusing — potentially even abusing — invasive vascular procedures, increasing patients’ chances of complications, which include amputation or even death.
They handed the federal agency a list of outlier physicians they found in the government insurer’s own data. But the agency has done little to stop the practice and instead continues to pay doctors who exhibit this behavior millions of dollars a year.
The names of the doctors were never publicly revealed.
ProPublica is shedding new light on the problem.
Working with data journalists from the health analytics group CareSet, and in consultation with experts, ProPublica sought to better understand how often physicians were using one particularly controversial procedure, the atherectomy, on patients with questionable need for it. Over the past year, ProPublica has chronicled the rise of these procedures along with horror stories of patients who lost their legs from complications.
Their cases and many others, plus dozens of interviews with patients, health care providers and medical device representatives, have laid bare a thriving industry of strip-mall clinics and outpatient vascular centers where elderly patients are being exploited for multimillion-dollar Medicare payouts.
As part of the procedure, doctors use a laser or bladed catheter to remove plaque from the patients’ vessel walls. For treatments conducted in outpatient clinics, Medicare pays generous reimbursements to doctors, who can charge tens of thousands of dollars for procedures done in a single visit. Experts recognize atherectomies are appropriate for severe vascular disease, but they told ProPublica that the majority of patients with milder symptoms like leg pain while walking, a condition known as claudication, should start with treatments like medication and exercise.
We analyzed Medicare claims records for people who had first-time atherectomies between 2019 and 2022 and found that nearly 1 in 4 patients underwent the invasive procedure after only a diagnosis for claudication, indicating an early stage of vascular disease.
This amounts to nearly 30,000 patients who may have undergone procedures too soon or possibly even unnecessarily. (Read more about our findings and methodology.)
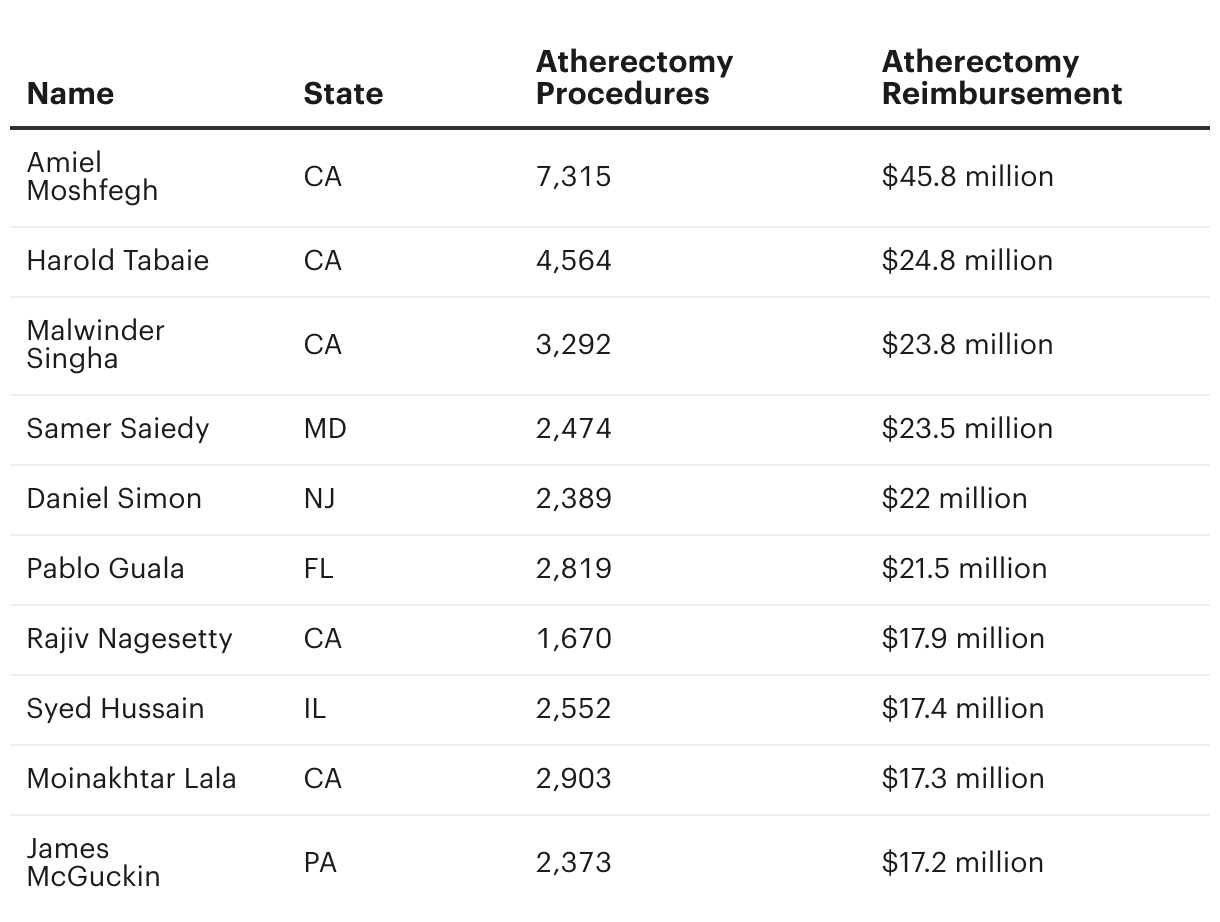
Some doctors stood out because of the money they made. Dr. Amiel Moshfegh, a Beverly Hills radiologist, received $45 million from Medicare over five years for performing thousands of atherectomies, according to public Medicare records. Most of his Medicare patients were older Latinos, according to federal data, who were warned in Spanish-language advertisements that poor circulation could lead to amputation. About 15% of his patients who underwent a first-time atherectomy, 170 of them, appeared to have milder disease based on their diagnosis for claudication, according to the data.
Other doctors stood out because a large portion of their patients who underwent atherectomies had just claudication, raising questions about the necessity of the procedures. That was the case for Dr. Christopher LeCroy, who works for a chain of vascular clinics across the Florida panhandle; about half of his first-time atherectomy patients appeared to have milder disease based on their diagnosis, according to the data.
And while over 5,000 physicians who provide vascular care rarely intervened on patients who appeared to have milder vascular disease based on their diagnoses, ProPublica and CareSet found that about 170 other doctors performed half or more of their first-time atherectomies on these kinds of patients.
“It’s concerning that we may be doing unnecessary procedures and spending unnecessary health care dollars,” said Dr. Caitlin Hicks, an associate professor of surgery at Johns Hopkins University School of Medicine and a leading researcher on procedure overuse. “We know that aggressive interventions for claudication may give short-term relief, but in the long term, patients are the same as they started or even worse.”
Doctors named in our data objected to being portrayed as part of the problem.
Moshfegh, for example, noted he had no malpractice claims or blemishes on his license. “Atherectomies ultimately can save the government and taxpayers millions of dollars by avoiding amputations,” he said. He did not respond to ProPublica’s questions on his clinic’s use of advertisements, the treatment of patients with milder vascular disease or why he had received more Medicare reimbursements for atherectomy than any other physician in the country. (Read his full statement here.)
LeCroy did not directly respond to ProPublica’s questions sent by email, but the clinical director at his practice said he doesn’t conduct procedures on patients with mild disease unless they have lifestyle-limiting pain and have already tried exercise and medication therapy. “This endovascular work is preventing patients having bypasses or amputation,” said Cherlynn Hecker. Others echoed these points.
Several portrayed the mounting concerns about overuse as part of a debate, not settled science, and said they should be trusted to decide whether their patients can benefit from atherectomies. Private practice doctors also explained that their high reimbursement payments are meant to cover their total business expenses and do not lead to excessive personal profit. Some rebuffed ProPublica’s analysis, taking issue with the use of claims data, which they said does not provide key details on patient symptoms and critiquing the focus on claudication, which they said can have a range of severity. While Medicare claims data has limitations, academics across the country and even government fraud detectives use it to examine trends and identify outliers.
Johns Hopkins surgeon and researcher Dr. Marty Makary said these kinds of outlier analyses are crucial to protecting patients. “Most of the public is flying blind,” said Makary, who also leads the organization Global Appropriateness Measures, which uses similar medical data to address outliers and curb overuse. “The moral dilemma that the medical community is now facing is that we can see practice patterns in big data that are inappropriate. Do we have a duty to act? I think we do.”
Using the research of Hicks, Makary and their colleagues as a springboard, ProPublica has spent the past year examining Medicare data for vascular care to answer some basic questions: Which doctors are making the most money off a single procedure? Who are they treating? And what is happening to their patients?
Relying on public Medicare data, we found that about 200 doctors are responsible for a majority of atherectomies conducted across the country. Over five years, from 2017 through 2021, this small cadre of mostly vascular surgeons, interventional radiologists and cardiologists has earned nearly $1.5 billion dollars, conducting almost 200,000 procedures. At the top of the list sits Moshfegh, the Beverly Hills radiologist who raked in almost double the reimbursements of any other doctor in America, for over 7,000 atherectomy procedures.
While some vascular specialists making millions have developed national empires of clinics, been profiled on local television or garnered dozens of online patient reviews, Moshfegh has kept a remarkably low profile.
After completing his medical training in 2014, Moshfegh went into outpatient vascular care. For a couple years, he led endovascular services for the Los Angeles office of Vascular Access Centers, a national chain of clinics founded by Dr. James McGuckin.
Moshfegh later began working with FIT Vascular, a smaller vascular clinic chain with offices in central Los Angeles and Bakersfield, California. He appears to have worked closely with several podiatrists, sharing hundreds of patients primarily with two podiatry clinics, according to recent Medicare referral claims data from CareSet. One of the podiatry groups, Stockdale Podiatry in Bakersfield, also shares office space with FIT Vascular — the vascular suite sits behind a beige, unmarked door off of the podiatry clinic’s waiting room.
When a ProPublica reporter visited the clinic, Victoria Arredondo, a medical assistant for FIT Vascular, told ProPublica that Moshfegh travels to Bakersfield from Los Angeles several times a week to conduct artery procedures, treating half a dozen patients a day. Nearly all of their patient referrals came from Stockdale Podiatry, she said. While Moshfegh’s name is not listed on FIT Vascular’s website, he is featured in its marketing videos and his face appears in its advertisements.
The federal government generally forbids doctors from making payments to induce referrals or making referrals to entities they have a financial interest in. While it’s not prohibited for physicians to pay another doctor to lease office space, such real estate transactions must be consistent with fair market value to abide by federal law. Neither Stockdale Podiatry or FIT Vascular responded to ProPublica’s emailed questions, including those related to their real estate arrangement. Moshfegh did not respond to ProPublica’s questions about his relationship with the podiatry clinic, though he did say that he adheres “the highest standards of medical ethics” and that his atherectomy statistics reflect “the confidence of referral sources in directing patients” to his practice.
While the raw numbers can highlight doctors like Moshfegh who stand out for how many atherectomies they do, they don’t provide much detail on how individual patients are being treated. So ProPublica worked with CareSet to look at the types of patients that doctors treat, examining whether doctors were frequently conducting procedures on patients who appeared to have more mild disease based on their diagnoses. Using Medicare claims data, we identified patients who underwent a first-time atherectomy procedure between 2019 and 2022, and for each doctor, we calculated the percentage of these patients who only had claudication.
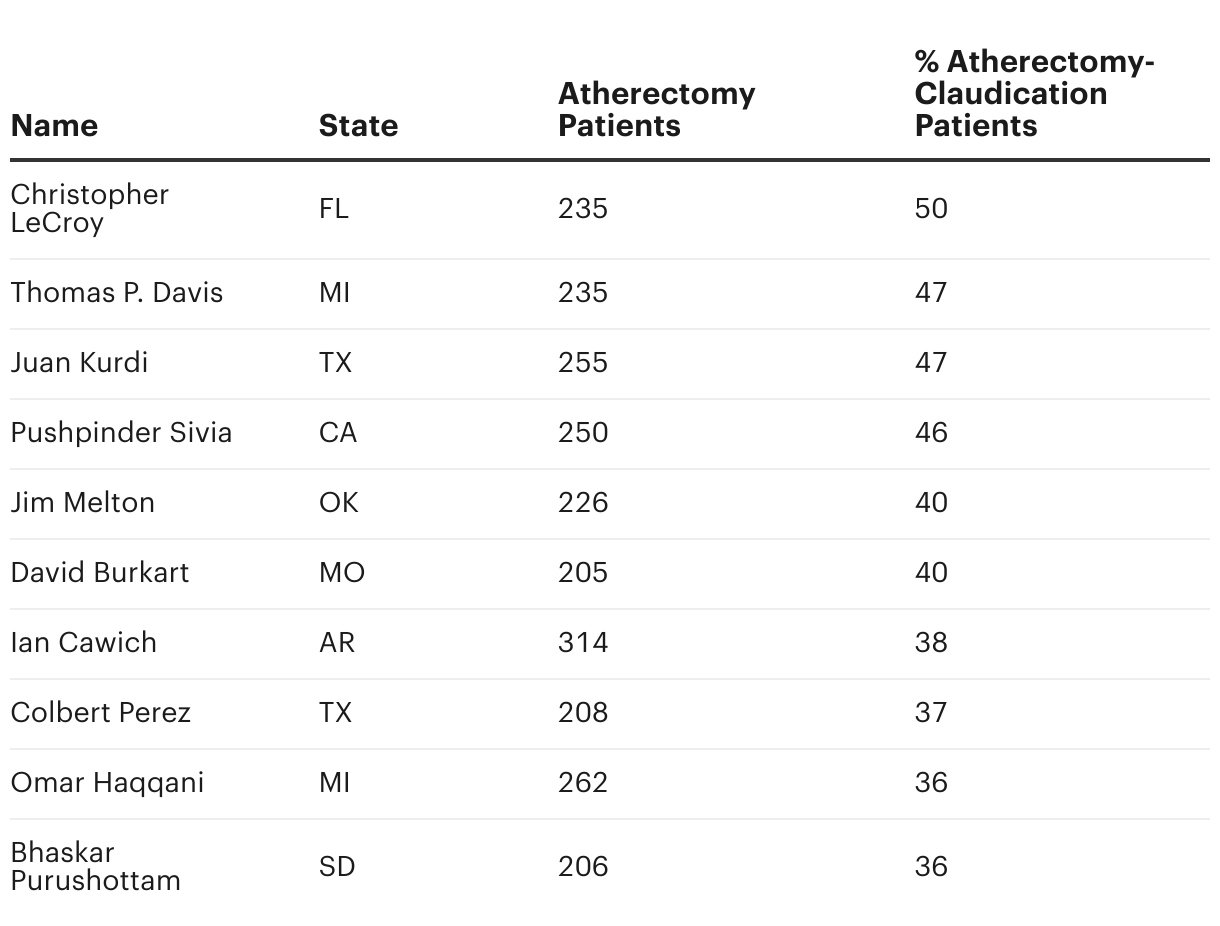
This highlighted doctors like Dr. Juan Kurdi of Lubbock, Texas; nearly half of his first-time atherectomy patients appeared to have milder disease based on their diagnosis, according to the data. Kurdi did not directly respond to ProPublica’s emailed questions or phone messages, and his lawyer declined to comment. Kurdi’s currently the target of a criminal investigation by the Department of Justice, according to court filings; he has not been charged. The government and his lawyers are discussing a potential pre-indictment resolution, according to case filings.
His colleague Dr. Colbert Perez, who was also high on this list with 37% of his first-time atherectomy patients having only claudication according to the data, said that their practice, Caprock Cardiovascular Center & Cath Lab, had been marking their patients with incorrect diagnosis codes in Medicare billing claims for several years, which made their patient population appear to have milder disease. While billing errors can occur, CMS mandates that physicians “are responsible for ensuring that claims submitted” under their name are “true and correct.”
Perez said that he rarely intervenes on patients with mild disease, following best practices, and said the center, which outsources its coding and billing to another company, was looking into the billing issue and was in contact with CMS for corrections and changes. He did not provide details on the federal investigation into Kurdi but told ProPublica that his colleague was “going through a separation” with the practice.
In all, experts who reviewed ProPublica’s analysis called the findings alarming and validating. They called on government insurers to do something about the fact that a quarter of all patients who got first-time atherectomies — enough to fit in a sports arena — may not have needed them. CMS told ProPublica that it monitors claims data for outliers and can act when it identifies problems, by denying claims, suspending payment or referring questionable providers to law enforcement.
“When we see patterns that are beyond the boundaries of reasonable according to respected peers in the field,” Makary said, “that is a signal that there should be a closer review.”
Editor’s Note
ProPublica reached out to every doctor named in our story through multiple emails and phone calls, providing questions to the physicians, clinics, hospitals or lawyers. The following doctors, their offices or lawyers did not respond to ProPublica’s questions for this story at the time of publication: David Burkart, Ian Cawich, Thomas P. Davis, Pablo Guala, Omar Haqqani, Syed Hussain, Juan Kurdi, Moinakhtar Lala, James McGuckin, Jim Melton, Rajiv Nagesetty, Daniel Simon, Pushpinder Sivia and Harold Tabaie. Dr. Bhaskar Purushottam and Monument Health, where he works, both declined to comment. Riverside Healthcare in Illinois, where Hussain has worked since September 2022, also declined to comment on the doctor’s practice.
In addition to the doctors quoted in the story, the following doctors responded to ProPublica’s findings.
Maryland vascular surgeon Dr. Samer Saiedy told ProPublica that Medicare claims data doesn’t include enough details to provide a full picture of why he may have treated a patient with an invasive procedure. At his practice, patients are only given the option of invasive procedures, he said, if they have severe pain and have already tried less aggressive approaches first. “If you look at atherectomy only, and you narrow down, yes, I’ll be an outlier because I do a lot of claudicants for severe symptoms after we do the medical treatment,” he said. “They cannot walk through the pain, they’re already on blood thinners, they’re already on this and already on this. We’re going to do something.”
Saiedy also said the Medicare reimbursement data is misleading. Saiedy, who has made about $23.5 million from Medicare in reimbursements for atherectomy procedures over five years, according to federal data, said the payments cover all clinic expenses and are not going to him directly. “You have to look at the overhead of the practice,” he said. “That includes nurses, anesthesia, leases for the equipment, rent.”
California interventional radiologist Dr. Malwinder Singha, who received $23.8 million in Medicare reimbursements for atherectomy procedures over five years according to federal data, echoed Saiedy’s concerns. “It is devoted to running of the [office-based laboratory] and only a tiny fraction is earned by the operator,” he wrote in an email to ProPublica. “I have to pay my employees and expenses for all the supplies (wires, balloons, stents, atherectomy catheters, etc.), imaging equipment, [electronic medical records], facilities rent, etc.”
Singha also took issue with the use of claims data to identify clinical outliers. "It does not take into account the patient population I see and the severity of their disease," he said. He added that outpatient facilities are safe, and their patients are satisfied with their care. "What I and my colleagues do is safe and effective," he said. "There are hundreds of office based labs who treat thousands and thousands of patients. The adverse event rate is miniscule."
Interventional radiologist Dr. James McGuckin, who received $17.2 million in Medicare reimbursements for atherectomy procedures over five years, treats “a significantly high-risk patient base” who are at-risk for amputation, said his attorney, David Heim, in an email this past August. Earlier this year, the Department of Justice sued McGuckin for submitting false claims to the federal health care programs for “medically unnecessary invasive peripheral artery procedures,” allegations that Heim had called “provably wrong.” His lawyers have moved to dismiss the case.









